Rickets and scurvy are deficiency diseases that result from inadequate metabolization of vitamins D and C, respectively. Scurvy results from an absence of sufficient vitamin C in the diet; whereas, rickets results from insufficient exposure to sunlight as much as from a dietary deficiency. Indeed, sufficient metabo-lization of vitamin D can be achieved simply through exposure of the skin to the ultraviolet light in sunlight. Lack of exposure or diminished exposure due to air pollution in industrialized urban centers of the nineteenth century became synonymous with the occurrence of rickets. Vitamin D is responsible for the maintenance of blood calcium and phosphorus levels, which are essential for normal endochondral (i. e., bone that forms from a cartilaginous precursor) bone formation. Without vitamin D, cartilage is not converted to bone mineral (hydroxyapatite). Rapidly growing infants and younger children are most at risk of developing rickets when the forces produced in Normal posture and movement cause bending in the poorly mineralized bones. Although all bones of the body can be affected, the most common features of the disease are mediolateral bending in the tibiae and fibulae and anterior bowing of the femora.
Although scurvy has become associated with long-distance sea voyages of the sixteenth to the nineteenth centuries, it is also found in industrialized nineteenth-century urban populations subsisting on an impoverished diet lacking in fresh fruit and vegetables or subsisting on only cooked meat (raw meat contains vitamin C, but it is destroyed in the process of cooking). Vitamin C is essential for collagen (the protein in bone responsible for its flexibility) and osteoid (bone matrix laid down by osteoblasts) production, as well as strong blood vessel walls. The major physical manifestation of vitamin C deficiency is hemorrhaging (bleeding). Because entheses are attached to the periosteum in infants and children, simple movements, even of the eye, and chewing causes bleeding which causes porous new bone formation (Figure 18). These formations are especially notable in the temporal fossae of the cranium, through which the temporalis muscles (the major muscles for mastication) pass, as well as in the jaws. Both of these diseases are found sporadically in earlier periods and their occurrence is often used as a population indicator of poor childhood health.
Although palaeopathologists encounter a number of other metabolic diseases in the course of population analyses, one of the most enigmatic and relatively commonly encountered is Paget’s disease or osteitis deformans, especially in European populations, which was first and famously described by Sir James Paget, who monitored the progression of the disease in a group of patients at the end of the nineteenth century. Despite its relatively common occurrence and distinctive physical manifestations, its cause remains obscure. Among the suspected etiologies is genetic predisposition, because it occurs in members of the same family, and exposure to paramyxoviruses, such as measles or canine distemper. The disease is progressive, affecting males over the age of 40 most commonly. It is characterized by diffuse porous bone formation with thickened cortical bone predominately of the axial skeleton (Figure 19), although bones of the appendicular skeleton can also be affected. The potential of palaeo-pathological studies to shed light on modern diseases comes in the form of a group of elderly males buried within a church and chapel associated with the Au-gustinian monastic house at Runcorn in Cheshire, England. Based on these individuals’ placements within the nave and chapel of the monastic church, locations normally reserved for those of high social

Figure 18 Fiber bone deposition in the orbits of a child due to the haemorrhaging (bleeding) of scurvy. These are bone-depositing lesions, unlike those in cribra orbitalia in Figure 5. Photograph courtesy of Jean Brown from the collections of the Biological Research Centre (BARC), University of Bradford.

Figure 19 The thickening of the cranial vault of Paget’s disease in the cranium of NP 21 from Norton Priory, Cheshire. Photograph courtesy of Dr. Alan R. Ogden, Biological Anthropology Research Centre (BARC), University of Bradford.
Standing (often families) in Medieval society, and the recovery of a coffin adorned with the family crest of the Haltons, an aristocratic family local to the area, these remains suggest that a genetic predisposition may be implicated in the disease etiology. The distribution of the lesions in these individuals demonstrates the variability of bone lesions that is a common feature of bone disease (Figure 20).
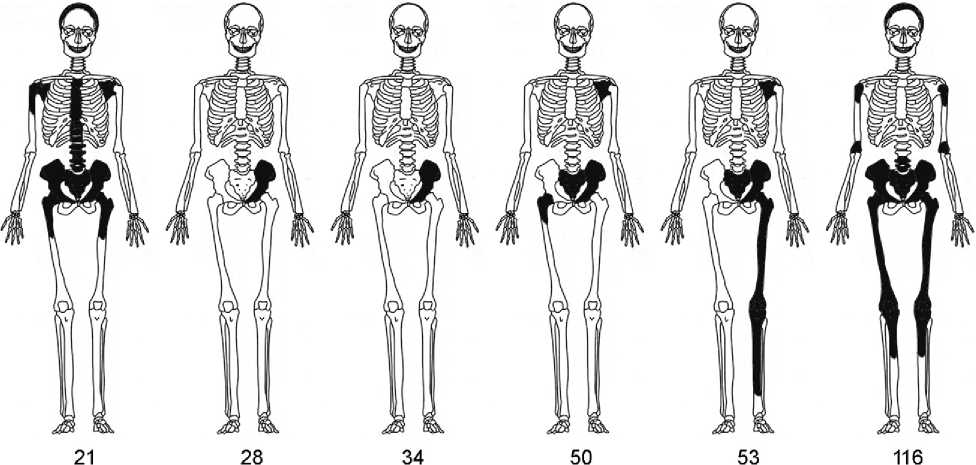
Figure 20 The variable pattern of Paget’s disease in six males buried intramurally at Norton Priory, Cheshire. NP 21 is thought to be Roger, brother of the third Baron Halton. Courtesy of Dr. Alan R. Ogden, Biological Anthropology Research Centre (BARC), University of Bradford.
 World History
World History