Types of Evidence from the Archaeological and Historical Records
In the field of archaeology it is possible to study health and disease through a number of avenues. These include palaeopathology, or the consideration of disease in skeletons and mummified bodies from archaeological sites (see Frozen Sites and Bodies); the study of artwork, such as sculpture, and illustrations on pottery or in paintings, which show people suffering from disease or being treated; descriptions of disease in historical written manuscripts; and the study of artifacts (e. g., medical and surgical instruments), ecofacts (e. g., medicinal plant pollen), and structural evidence (e. g., the remains of hospitals). Some of these avenues are plentiful and unambiguous while others can be very difficult to analyze and interpret. For example, written accounts of disease may be influenced by the author’s preferences and interpretation of events, which may bear no resemblance to the facts of the time. Furthermore, signs and symptoms of a number of diseases may be similar and therefore difficult to differentiate when described. For example, tuberculosis, chronic bronchitis, lung cancer, and pneumonia may all induce breathlessness and coughing up blood. Artistic representation can also be ambiguous, for example, when a rash is depicted, a sign that can equally apply to many diseases such as leprosy and smallpox. Likewise, the study of human skeletal remains may provide only a basic understanding of what diseases were prevalent at a certain point in time because not all diseases affect the skeleton, and few bodies with preserved soft tissue are found in archaeological contexts. Thus, some evidence is more useful for some diseases than others. In addition, the different types of evidence for disease may be more commonly found in different temporal and geographic contexts. For example, it is only when urban centers develop that we see more organized attempts to control and treat disease, with the founding of hospitals and the manufacture of surgical instruments.
Methods of Study of Human Remains
The study of cremated and inhumed human remains from archaeological sites provides the primary evidence for disease, and the funerary contexts from which they derive vary both spatially and temporally. For example, in the Neolithic of Europe chambered cairns predominate, often with mixed burials, while later in the Medieval period discrete burials in large cemeteries are the norm; this makes analysis of disease from different contexts challenging (see Burials: Dietary Sampling Methods). Methods of identification of human remains include visual/ macroscopic, histological, radiographic, and biomolecular techniques, with the majority of evidence coming from macroscopic analysis in the last 10 years, the use of biomolecular methods such as the extraction and amplification of DNA from specific disease-causing organisms has enabled the identification of soft tissue disease in skeletal remains, such as plague and malaria, and the presence of disease in people who have died before bone changes occurred. For example, plague DNA has been found in the teeth of skeletons from post-Medieval plague pits in southern France. Most research on palaeopathology is focused on the most commonly found human remains on archaeological sites, skeletons and, generally speaking, for many parts of the world, smaller numbers of prehistoric burials have been found than for later periods. This might reflect differences in disposal of the dead (e. g., cremation vs. inhumation), and the ability of archaeologists to find the evidence. However, the survival of buried bodies depends very much on the burial environment, and this also determines whether whole bodies survive to be excavated.
For example, hot and cold (dry) environments preserve bodies well, including soft tissue, but there are relatively few mummified bodies available for analysis compared with skeletal remains.
Categories of Disease Identifiable
The evidence for disease in skeletal remains can be categorized into congenital, dental, joint, infectious, circulatory, metabolic, endocrine, neoplastic, and trauma, with the dental, joint, infectious, and trauma categories providing more abundant evidence. Thus, it is therefore clear that many diseases are absent when compared with the suite of health problems affecting human populations today. Stature, however, is also a good indicator of health because it is in the growing years when an adequate well-balanced diet and freedom from disease are essential for populations to attain their optimal height for their age, sex, population, geographic location, and time period. In adults, unless a medical complaint is affecting height, reduced height usually indicates a chronic dietary deficiency or disease. A number of studies of children’s skeletons have also indicated that reduced growth of bones is usually seen in skeletons with a number of indicators of stress such as dental enamel defects, and children with shorter bones are seen to die younger in the past.
Congenital disease may be genetic or nongenetically initiated and includes conditions such as spina bifida and cleft palate, and dental disease tells us something about diet, childhood stress, occupation, dental care, and dentistry. For example, recent research on skeletons from Bahrain shows few caries, which may reflect the naturally high fluoride levels in drinking water protecting the teeth. Identification of how people may use their teeth for particular activities has also shown us, through particular wear patterns, that people from post-Medieval England smoked pipes and held nails in their teeth for carpentry, and that nineteenth-century Inuit Eskimo women held animal skins in their front teeth to stretch and soften them to make into clothes. Trauma gives us an indication of domestic and interpersonal violence, along with efforts made to treat injuries, and joint disease can show the process of aging and the effects of work on the joints. For example, research on skeletons from the fifteenth-century English battlefield site of Towton found many with unhealed injuries to their skulls (around four per skull), supporting historical documentation for the site of the battle. Infections may be nonspecific (we do not know what specific organism caused the infection) or specific (where we do, e. g., Mycobacterium leprae is the organism causing leprosy) and may inform us about levels of hygiene, living conditions, population density, trade, and the keeping of animals and the consumption of their products. Brucellosis and tuberculosis are both infections that can be contracted by humans from their infected animals by ingesting or working with their infected products. The first evidence for tuberculosis comes from Italy, dated to the Neolithic, and probably relates to domestication of animals. Many examples of tuberculosis have been identified in the archaeological record (Figure 1) but, in contrast, few records of brucellosis have been reported: some examples derive from Herculaneum, Italy and date to AD 79 when Mount Vesuvius erupted and preserved the site under volcanic ash. Sixteen of the 151 individuals had evidence of brucellosis in their skeletons and it was also identified in preserved dairy products. Circulatory disease tells us about problems of the normal circulation of the blood around the bodY which may impact on the skeleton, and disorders of the metabolism and endocrine system (metabolic and endocrine disease) such as Scurvy and thyroid problems, respectively, may help us understand dietary and other deficiencies. For example, osteoporosis has been identified in individual skeletons (e. g., sixth-century Negev Desert in Israel) but also in larger groups of burials (see Osteological Methods; Figure 2). A recent study found a higher rate of bone loss in a Medieval population in England than today which was surprising considering the (assumed) more active lifestyle of the past. While neoplastic and congenital disease is uncommon in the archaeological record, evidence may suggest that increasingly complex societies develop more of these conditions. For example, in Britain there is very scarce evidence in prehistory but this increases from the Roman period onwards; pollutants in the atmosphere and a more complex diet may be predisposing people to tumors and congenital disease (Figure 3). While many diseases can be recognized, the reader should be aware that poor sample representivity (making results ambiguous), the inability to age adult skeletons accurately and sex nonadult skeletons (making demographic profiles incomplete), pseudopathological lesion differentiation, the problem of identifying specific diseases beyond the disease category, and the lack of ability to identify soft tissue diseases without the use of ancient DNA analysis (also fraught with problems) make the study of health and disease in skeletal remains very challenging. Added to this are the limited ways in which the skeleton can react to disease (bone formation and destruction, in particular skeletal pattern, based on clinical data).
Figure 2
England.
Compression fractures of vertebrae: Early Medieval

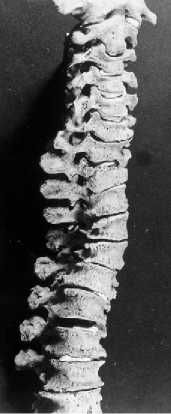
Figure 1 Tuberculosis of the spine: Early Modern period, North America.

Figure 3 Tumor on fibula from Early Medieval England.
Disease within Its Cultural Context
Bound up with the evidence of disease is the necessary consideration of that evidence in context. A population’s general living environment (inside and outside the home), the climate and weather patterns, levels of hygiene, cleanliness of food and water supply, what work they do, and who and what they come into contact with, plus their biological sex, age, social status, and ethnicity, all affect what diseases they might contract. Studying disease for its own sake and in isolation from the context from which the evidence comes makes its analysis and interpretation incomplete. The quality and quantity of food and a balanced diet is particularly important in developing a strong immune system to withstand disease. Until relatively recently, it has only been possible to detect dietary deficiencies in skeletal remains, but stable isotope analysis of carbon, strontium, and nitrogen in teeth and bones can now allow us to assess the tYpes of plants eaten and the contribution of marine and terrestrial animals to the diet (see Stable Isotope Analysis). For example, in Portugal more plant and animal domesticates were being eaten in the Neolithic compared to the Mesolithic, and in the Mesolithic and Early Neolithic Ukraine hunting, fishing, and gathering provided the protein component of the diet, but there was an increase in fish consumption in the later Neolithic. By looking at the details of dietary intake, it becomes possible to assess whether diet was a contributory factor to health or disease for our ancestors.
It is also necessary to understand that concepts of health, disease, and how disease should be treated, vary today around the world and between developed and developing countries. For example, Graeco-Roman medicine considered divine displeasure as a major cause of disease and, while Roman medicine advocated a preventive approach to health by regulating food and drink, taking regular exercise, massages, baths, and relaxation, it also utilized herbal remedies alongside the influence of gods, goddesses, and magical remedies for treating disease. It is therefore important to understand that how populations deal with disease can vary considerably both temporally and geographically.
 World History
World History